
Ventilator vs. Tracheostomy: A Guide for Caregivers
- Opulent Private Care Services

- 3 days ago
- 9 min read

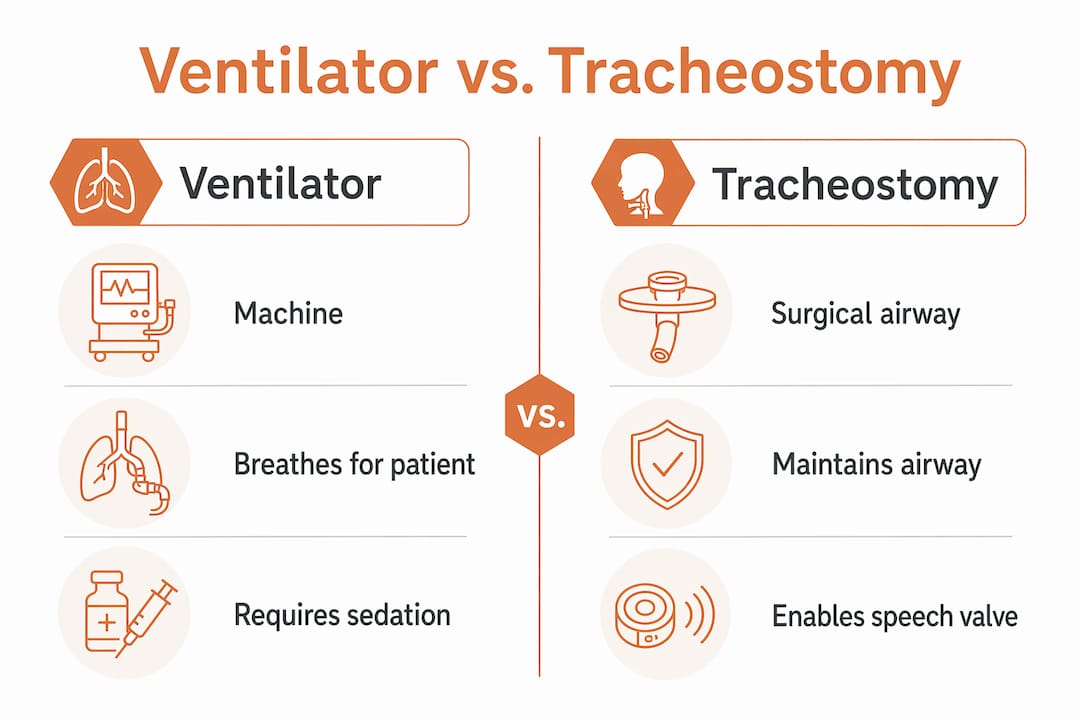
A ventilator is a machine that mechanically moves air in and out of the lungs, while a tracheostomy is a surgically created opening in the neck that provides a stable airway. Understanding the difference between ventilator and tracheostomy care is one of the most important things a family can do when a child faces a serious respiratory condition. These two interventions are not the same thing, though they often work together. A child may have a tracheostomy without needing a ventilator at all, or may rely on both simultaneously. Knowing which does what shapes every care decision that follows.
What is the difference between a ventilator and a tracheostomy?
A ventilator and tracheostomy serve completely different functions, even though they frequently appear together in pediatric respiratory care. A ventilator is a device. A tracheostomy is a surgical procedure that creates an opening. One breathes for your child; the other provides the route through which breathing can happen.

The confusion is understandable. Both show up in intensive care settings, both involve tubes, and both relate to breathing. The key distinction is that a ventilator replaces or assists the mechanical act of breathing, while a tracheostomy simply creates a more stable, direct path to the airway. A child with a tracheostomy who breathes independently does not need a ventilator. A child on a ventilator may breathe through a standard oral tube or through a tracheostomy tube, depending on how long ventilator support is expected to last.
Opulentprivatecare works with families navigating exactly this distinction every day. Families who understand the difference make better decisions, ask sharper questions, and feel less blindsided when care plans shift.
How does a ventilator support a child’s breathing?
Ventilators mechanically move air in and out of the lungs for patients who cannot breathe adequately on their own. The machine delivers pressurized air, often with added oxygen, through a tube placed in the airway. The child’s lungs inflate and deflate according to settings the medical team programs into the machine.
Pediatric ventilators offer several modes of support:
Full control mode: The machine delivers every breath. The child makes no breathing effort.
Assist-control mode: The ventilator delivers a set number of breaths per minute but also responds when the child tries to breathe.
Pressure support mode: The child initiates each breath, and the ventilator adds extra pressure to make each breath easier.
CPAP (Continuous Positive Airway Pressure): The machine holds the airway open with constant pressure, but the child breathes independently.
Ventilators are used when a child has acute respiratory failure, chronic lung disease, neuromuscular weakness, or any condition that makes independent breathing unsafe or exhausting. The settings, including respiratory rate, tidal volume, and oxygen concentration, are adjusted based on the child’s blood gas results and clinical response.
Pro Tip: Ask the medical team to explain which ventilator mode your child is using and why. Understanding the mode tells you a great deal about how much breathing work your child is doing independently.
The ventilator connects to the airway through either an endotracheal tube placed through the mouth, or a tracheostomy tube placed through the neck. Short-term ventilation typically uses an oral tube. When ventilation extends beyond a week or two, the team will usually discuss switching to a tracheostomy.
What is a tracheostomy and why is it recommended?
A tracheostomy involves creating a surgical airway through an incision in the front of the neck, below the vocal cords. A tracheostomy tube is then placed through that opening directly into the trachea. The term “tracheotomy” refers to the surgical act of cutting; “tracheostomy” refers to the resulting opening. In everyday clinical use, the terms are often used interchangeably.
Pediatric tracheostomies are recommended for several distinct reasons:
Prolonged ventilation: When a child needs mechanical breathing support for more than 10–14 days, a tracheostomy is more comfortable and safer than keeping an oral tube in place.
Upper airway obstruction: Conditions like subglottic stenosis, laryngomalacia, or tumors can block the natural airway. A tracheostomy bypasses the obstruction entirely.
Secretion management: Children who cannot clear mucus effectively benefit from the direct airway access a tracheostomy provides for suctioning.
Neurological conditions: Children with brain injuries or neuromuscular diseases often need long-term airway protection.
The tracheostomy tube itself does not breathe for the child. It simply holds the surgical opening patent so air can pass in and out. If the child breathes well enough on their own, no ventilator is needed. If not, the ventilator connects directly to the tracheostomy tube.
Pro Tip: Tracheostomy tubes come in different sizes and styles. Ask the care team for the exact tube brand, size, and inner diameter your child uses. Keep this information written down and accessible at home for any emergency.
Tracheostomy carries risks including bleeding, infection, accidental decannulation (tube coming out), and tracheal stenosis over time. These risks are manageable with proper training and consistent care, but families need to know they exist before agreeing to the procedure.
How do ventilators and tracheostomies work together?
The clearest way to understand ventilator vs. tracheostomy is to think of them as separate tools that often work as a pair. The tracheostomy is the door. The ventilator is the engine. A child can have the door without the engine, but the engine always needs a door.
Feature | Ventilator | Tracheostomy |
What it is | A machine | A surgical airway |
Primary function | Delivers or assists breaths | Provides stable airway access |
Required for breathing? | Yes, when lungs cannot function | No, child may breathe independently |
Duration of use | Acute or chronic | Often long-term |
Connection point | Oral tube or tracheostomy tube | Directly in the neck |
Clinical guidelines recommend considering tracheostomy for patients who have been ventilated for 10–14 days. That recommendation exists because oral intubation becomes increasingly uncomfortable and risky the longer it stays in place. A tracheostomy at that point is not a sign of failure. It is a deliberate step toward stability.
Tracheostomies facilitate ventilator weaning by reducing the need for heavy sedation, allowing the child to be more alert and participate in physical therapy. Some children with tracheostomies can eat, drink, and even speak with the right valve in place. That level of function is rarely possible with an oral endotracheal tube.
Pro Tip: A Passy Muir Valve (PMV) is a one-way speaking valve that fits over the tracheostomy tube. Ask the speech-language pathologist whether your child is a candidate. Even brief periods of voice can significantly support development and family connection.
One important risk to understand: a tracheostomy bypasses natural airway defenses, which increases the risk of infection, including ventilator-associated pneumonia. Meticulous site care and suctioning technique are not optional. They are the primary way families protect their child from this complication.
What are the long-term caregiving responsibilities for families?
Managing a child with a tracheostomy and/or ventilator at home is a full-time commitment. Families who go in prepared handle the transition far better than those who are surprised by the scope of daily care.
Tracheostomy site care: Clean the skin around the stoma daily. Change the tracheostomy ties regularly to prevent skin breakdown. Watch for redness, swelling, or discharge that signals infection.
Suctioning: Children with tracheostomies cannot cough secretions out the way other children can. Caregivers must suction the tube on a schedule and whenever the child shows signs of distress or noisy breathing.
Ventilator management: Learn every alarm on the machine and what each one means. Know the difference between a low-pressure alarm (possible disconnection) and a high-pressure alarm (possible blockage or coughing).
Emergency preparedness: Keep a spare tracheostomy tube of the same size and one size smaller at the bedside at all times. Practice tube changes until the process is automatic.
Feeding and speech: Many children with tracheostomies work with speech-language pathologists and feeding specialists. Coordinate these therapies early, not after problems arise.
Psychosocial support: Caregiver burnout in families managing pediatric tracheostomy and ventilator care is real. Seek respite care, connect with parent support groups, and accept help when it is offered.
Opulentprivatecare provides specialized tracheostomy and vent support for families in Georgia, including hands-on training and consistent nursing coverage so caregivers are never managing alone.
What does research say about timing and outcomes?
Early tracheostomy, defined as within 14 days of intubation, does not significantly reduce mortality compared to later tracheostomy. A meta-analysis of 9 randomized controlled trials covering 2,500 patients found that early tracheostomy may shorten the duration of mechanical ventilation and increase ventilator-free days at 90 days, but it does not change survival rates. That finding matters because families sometimes believe that getting a tracheostomy sooner will save their child’s life. The evidence says the timing is less important than the quality of care that follows.
“Tracheostomy decisions should be individualized. Families must understand it is an airway management tool with real benefits and real limitations. It does not guarantee a shorter hospital stay or resolution of respiratory failure.” — Clinical guidance on tracheostomy timing
Transitioning from an oral tube to a tracheostomy is best understood as buying time for recovery when ventilator weaning attempts have not succeeded. It creates a more stable platform for rehabilitation, not a cure. Families who hold that framing tend to set more realistic expectations and engage more productively with the care team.
Key Takeaways
A ventilator is a machine that breathes for a child, while a tracheostomy is a surgical airway that provides access for breathing support, and the two serve distinct but often complementary roles in pediatric respiratory care.
Point | Details |
Ventilator vs. tracheostomy | A ventilator is a device; a tracheostomy is a surgical airway. They are not interchangeable. |
Tracheostomy timing | Guidelines suggest considering tracheostomy after 10–14 days of ventilation for comfort and stability. |
Independent breathing possible | A child with a tracheostomy may breathe without a ventilator if lung function allows. |
Infection risk is real | Tracheostomies bypass natural defenses; daily site care and suctioning reduce pneumonia risk. |
Early tracheostomy and mortality | Research shows early tracheostomy does not reduce mortality but may shorten ventilation duration. |
What I have learned from families navigating this decision
Families come to us at Opulentprivatecare after some of the hardest conversations of their lives. A doctor has just explained that their child needs a tracheostomy, or that the ventilator may be permanent. The medical facts are delivered clearly, but the emotional weight lands differently.
What I have seen consistently is that the families who do best are not the ones who accept every recommendation without question. They are the ones who ask exactly what each intervention does, what it does not do, and what daily life will look like six months from now. The question “is a tracheostomy better than a ventilator?” does not have a universal answer. It depends entirely on the child’s diagnosis, trajectory, and what the family can realistically sustain at home.
The families I respect most treat the medical team as partners, not authorities. They push back when something does not make sense. They ask for the evidence. They also recognize when they need help and ask for it before they are exhausted. Home nursing care is not a luxury in these situations. For many families, it is what makes the difference between a child thriving at home and a child returning to the hospital repeatedly.
The benefits of pediatric home care go well beyond convenience. Consistent, trained nursing support at home reduces complications, supports caregiver wellbeing, and gives children the best possible environment for development. That is not a sales point. It is what the evidence shows.
— Opulent
Pediatric respiratory care at home with Opulentprivatecare
Families managing a child’s ventilator or tracheostomy care at home need more than equipment. They need a nurse who shows up, knows the child, and handles emergencies with confidence.
Opulentprivatecare provides in-home pediatric nursing in Georgia for children with tracheostomies, ventilator dependence, and complex respiratory needs. The “3 Thumbs Up Rule” means every placement requires approval from the family, the nurse, and Opulentprivatecare before care begins. That process produces a consistent caregiver, not a rotating roster of strangers. Opulentprivatecare publishes shift fill rates and nurse retention metrics so families can evaluate reliability before committing. Reach out to learn whether your child qualifies for in-home nursing support.
FAQ
What is the main difference between a ventilator and a tracheostomy?
A ventilator is a machine that assists or replaces breathing, while a tracheostomy is a surgically created opening in the neck that provides airway access. A child may have one without the other.
Can a child with a tracheostomy breathe without a ventilator?
Yes. A tracheostomy provides an airway but does not breathe for the child. If the child’s lungs function adequately, no ventilator is needed.
When do doctors recommend a tracheostomy over continued intubation?
Clinical guidelines recommend considering tracheostomy after 10–14 days of mechanical ventilation, because prolonged oral intubation increases discomfort and complication risk.
Does getting a tracheostomy earlier improve survival?
Research shows early tracheostomy does not significantly reduce mortality. It may shorten the duration of mechanical ventilation, but survival outcomes depend on the underlying condition and overall care quality.
What are the biggest risks families should know about tracheostomy care at home?
The primary risks are infection, accidental tube displacement, and tracheal stenosis. Infection risk increases because the tracheostomy bypasses the body’s natural airway defenses, making daily site care and proper suctioning technique critical.
Recommended
Comments